Comfort Aid
A patient transfer system for Indian public hospitals that gets rid of the risks that come with manual bed-to-stretcher transfers. No lifting, no improvised bedsheet methods, and ideally just one caregiver needed.
Developed through immersive field research at AIIMS New Delhi, following the Design Thinking process: Empathise → Define → Ideate → Prototype → Test.
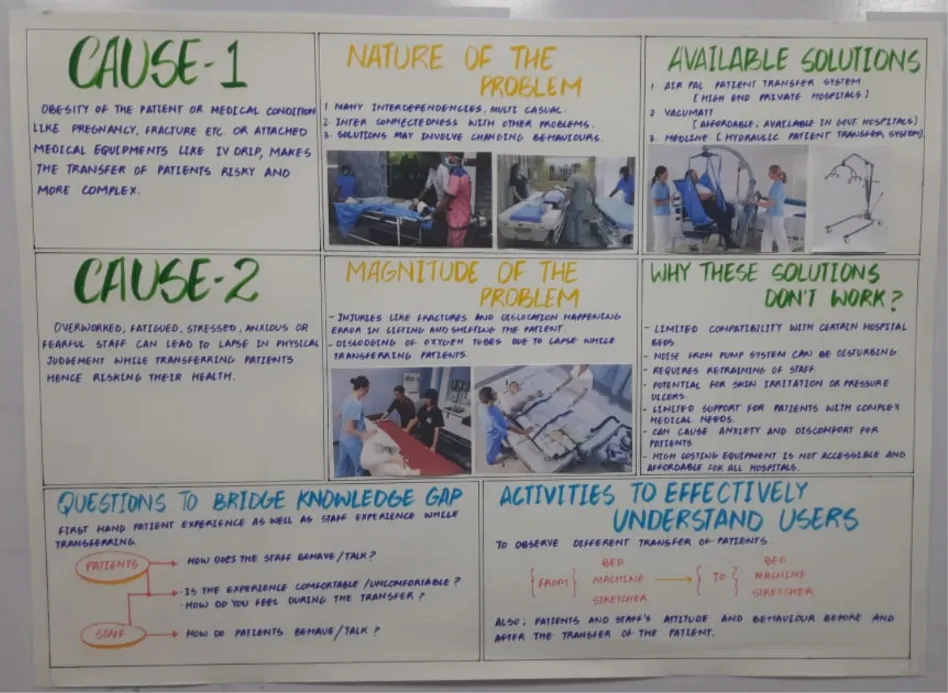
The Problem
Manual transfer was never designed.
The most common method is lifting a patient using bedsheets, with two to four staff coordinating the move. This came about out of necessity in under-resourced settings and stuck around because no better option was accessible or affordable.
In high-pressure wards like emergency and trauma departments, the number of transfers per shift makes it almost impossible for nurses to be careful every time. Even the ones who know the right technique don't always have the time to use it.
- Physical pain during transfer, particularly for post-surgical and trauma cases
- Risk of further injury to spine, limbs, and open wounds
- Psychological distress from undignified handling
- Acute spinal loading from coordinated vertical lifts
- Cumulative musculoskeletal injury over months of daily transfers
- Mental burden from complex coordination under time pressure
Field Research
Two days at AIIMS New Delhi.
We spent two days on immersive field observation and structured interviews across Emergency, Trauma, Oncology, Neurology, NICU, and Pediatrics. Covering multiple departments was intentional. Transfer challenges look quite different depending on the patient type and ward.



“Where do we find the time to carefully transfer a single patient when there are five others waiting for immediate attention? In a place like the trauma center, with such a heavy workload, it is hard to keep everything straight in your head.”
“Here, we usually have two or three people available to assist with patient transfers, but this is AIIMS. The real challenges are in rural hospitals, where it is often the relatives who are instructed by the staff themselves to move patients — and that is where most accidents occur.”
Research Synthesis
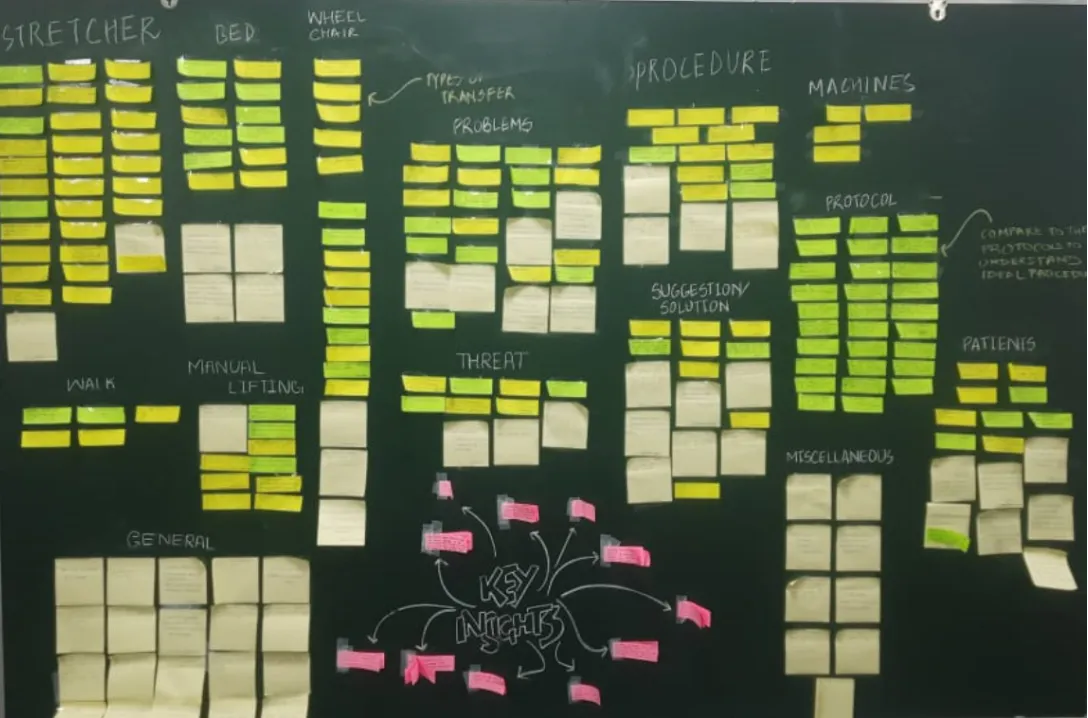
Affinity Mapping.
After the visit, we transcribed everything and ran an affinity mapping session across twelve categories: Stretcher, Bed, Wheelchair, Patient, Problems, Threats, Procedure, Protocols, Suggestions, Manual Lifting, General, and Miscellaneous.

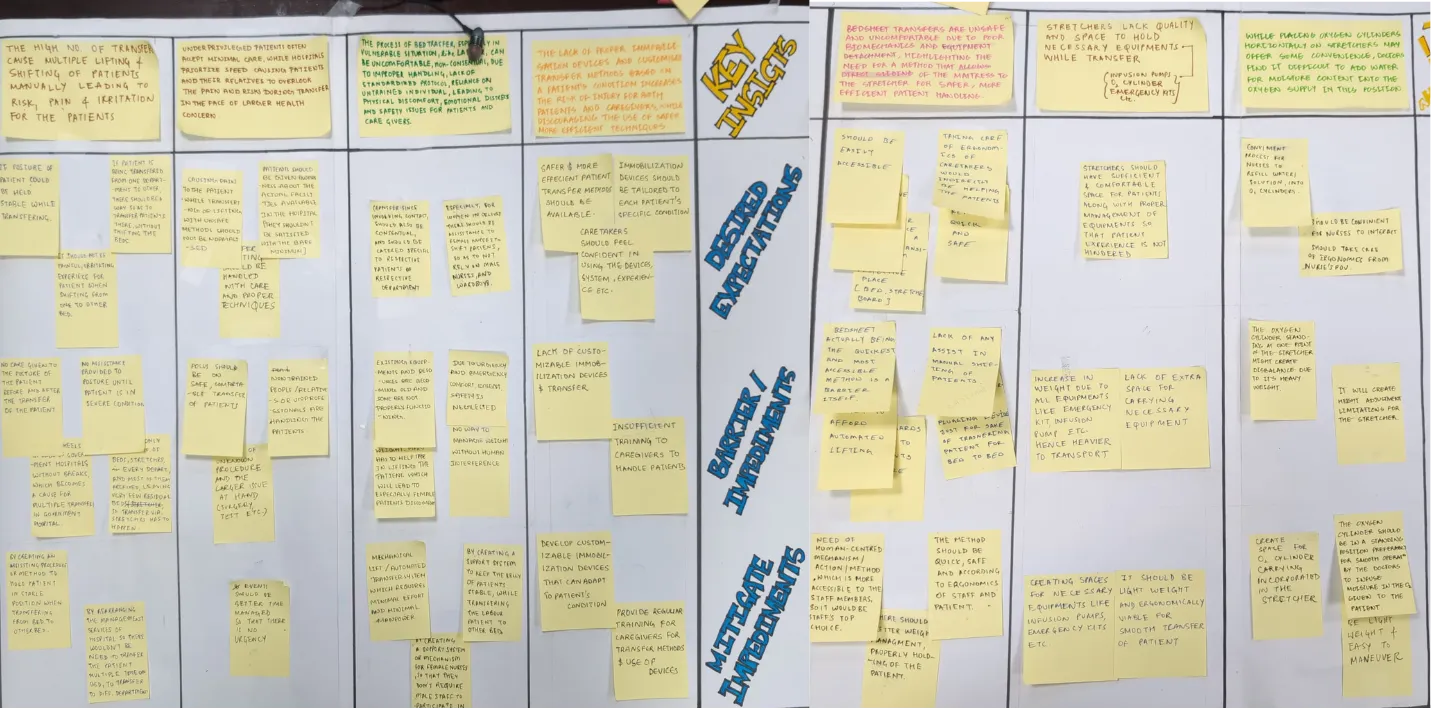
Five Problem Clusters
The number of lifts in a single shift is what makes it dangerous. No individual lift is the problem. It's the cumulative load across hundreds of shifts, over an entire career.
Pregnant women, post-surgical patients, and trauma cases carry the most risk. The bedsheet method doesn't adjust for any of that. A stable patient and a critically vulnerable one get handled the same way.
Safe transfer protocols do exist. They just aren't followed in practice. The correct procedure takes more time and more staff than most public wards can realistically spare.
The stretchers we observed weren't designed with the full transfer process in mind. There's nowhere to put IV lines, oxygen cylinders, or monitoring equipment, so staff attention is constantly split.
There's no standard method for keeping specific body parts still during a lateral transfer. The spine, neck, and injured limbs are all at risk when the only mechanism is a bedsheet.
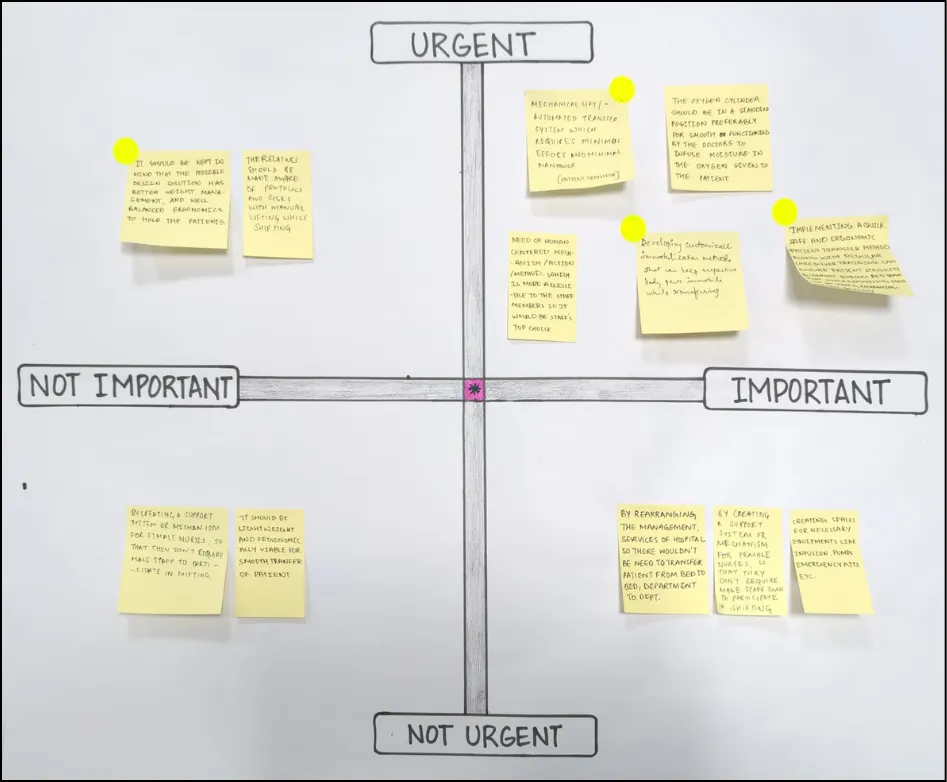
Key Insight-to-Action Priority Matrix, translating research findings into design requirements

User Persona
Rajni, 26
Construction labourer · Tier-2 city, Northern India · 4 months pregnant
Rajni sits at the intersection of the three highest-risk factors we identified: clinical vulnerability from her high-risk pregnancy, the constraints of an under-resourced public hospital, and limited health literacy that makes it hard for her to push back on how she's being handled, even when something feels wrong.
A solution that keeps Rajni safe without requiring her to ask for better care, or her caregivers to spend extra time, is one that actually fits the constraints of the system. That's the kind of design that holds up in practice.
How Might We
“How might we design a system that's easier on both staff and patients, reduces the physical load, allows for some customisation around patient stabilisation, and is actually the option that hospital staff want to use in Indian public healthcare settings?”
Ideation
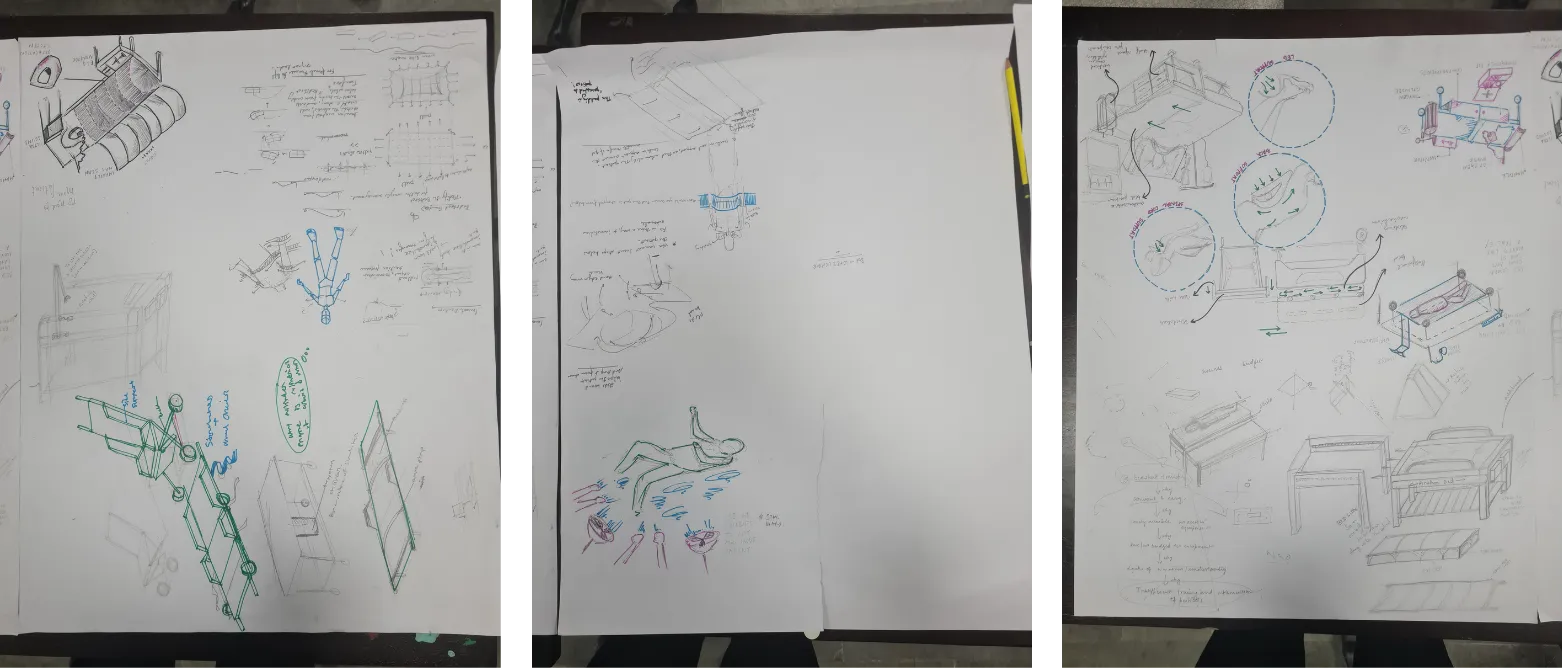
SCAMPER to concept.
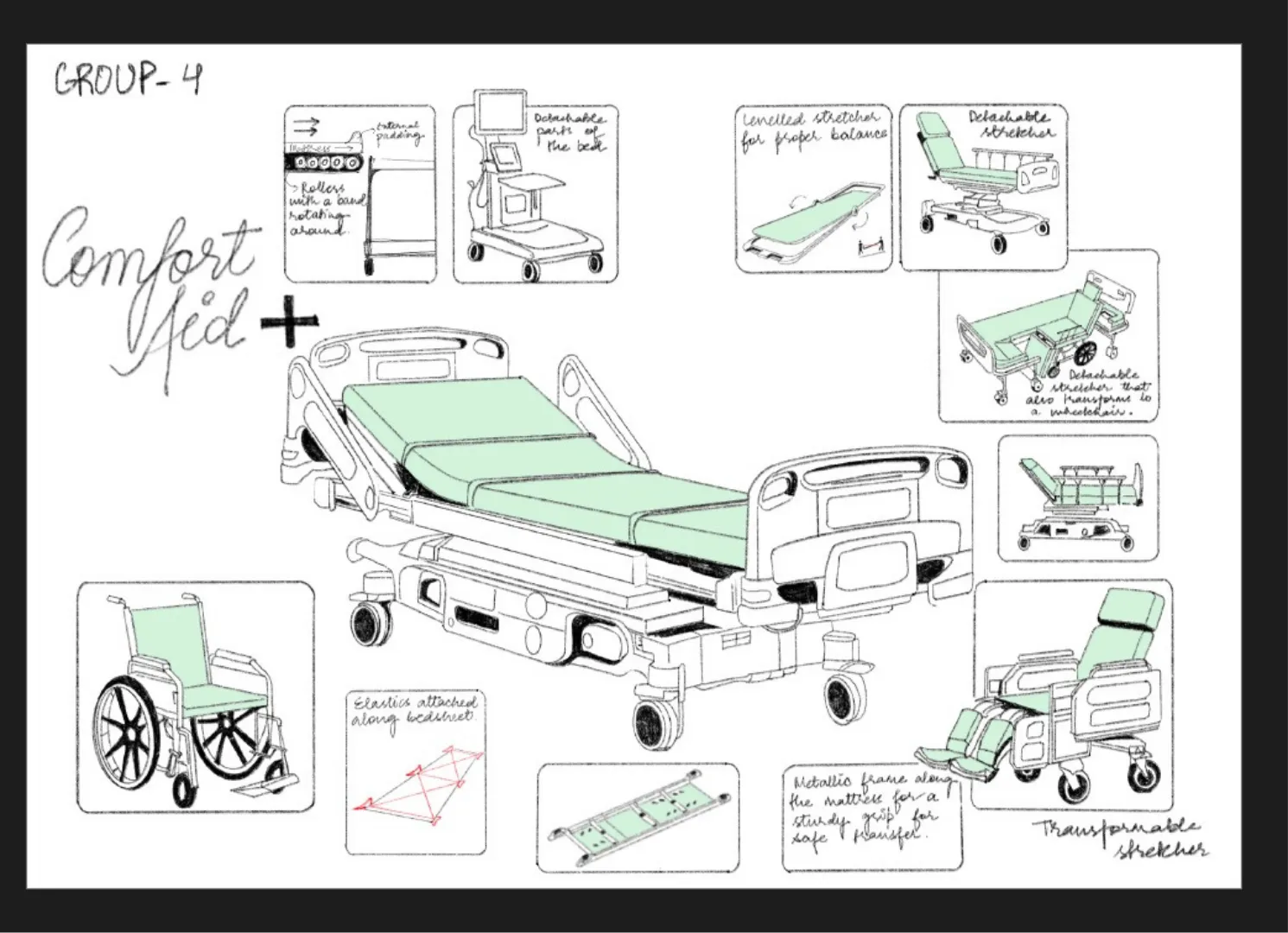
Three of our SCAMPER directions kept pointing toward the same idea: a mattress that slides along a rail between the bed and the stretcher. The patient stays on the mattress throughout. The mattress is the transfer mechanism.
Replace manual lifting entirely with a lateral sliding mechanism. This ended up being the core principle behind the final concept.
Add snap-fit alignment feedback so the bed and stretcher are correctly positioned before the transfer even begins.
Get rid of the vertical lift completely. If the mattress moves from the bed to the stretcher, there's nothing left to lift.
Adjust the mattress profile for different body types and vary the sliding resistance based on patient weight to keep the motion controlled.
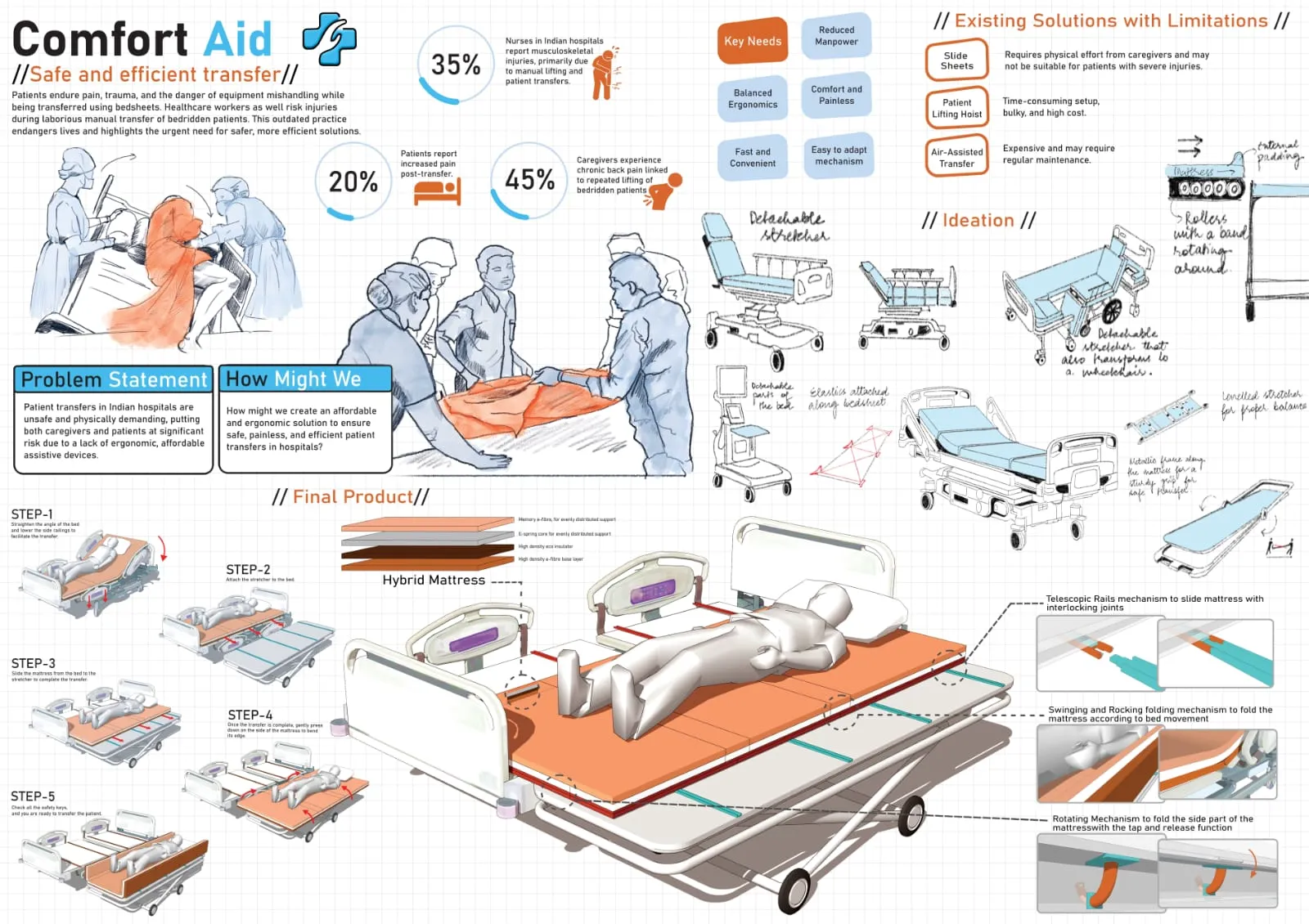
The Solution
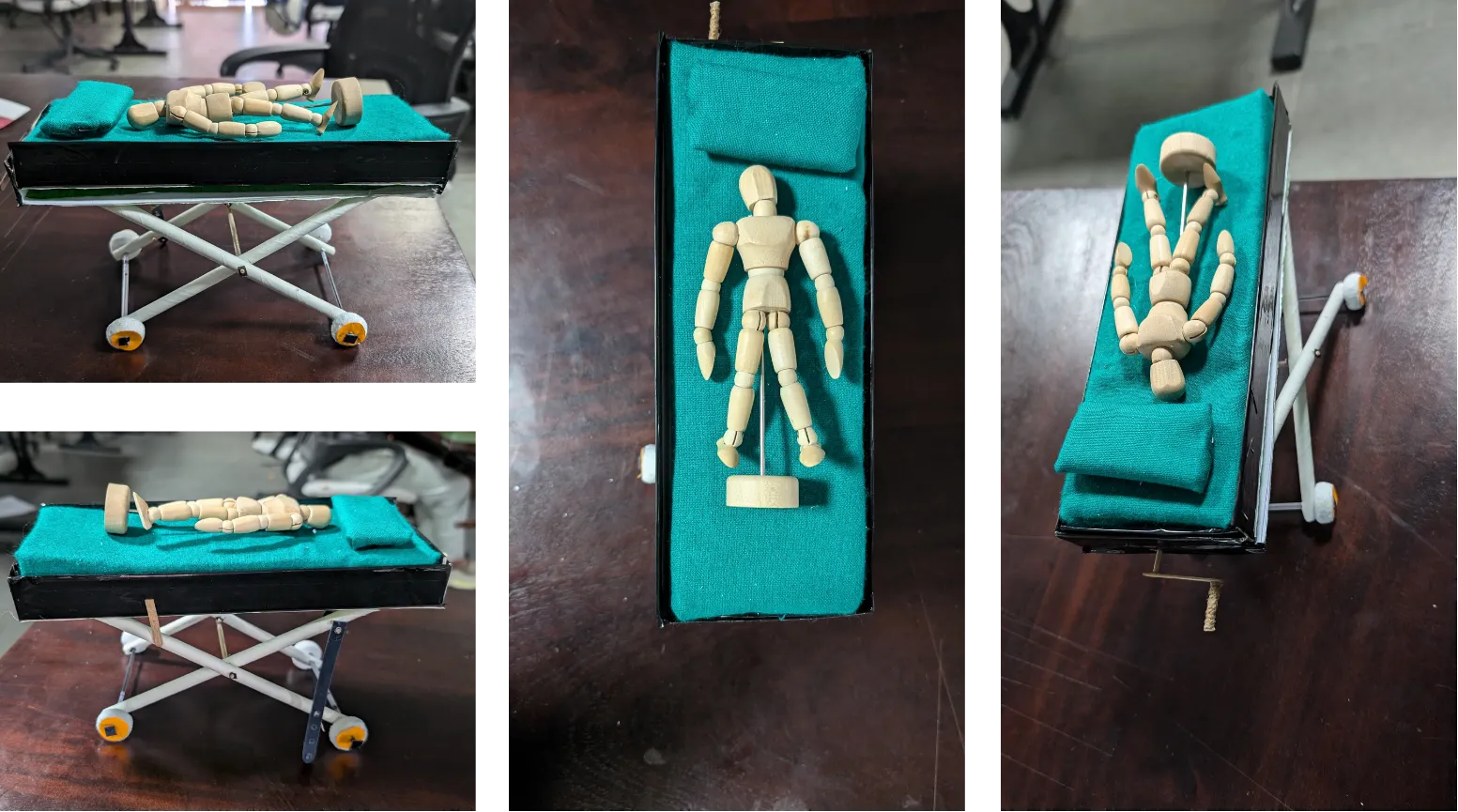
A hybrid slide-mattress system.
ComfortAid is a hybrid slide-mattress on a telescopic rail system. The patient never moves relative to the mattress. The mattress itself slides from the bed to the stretcher, carrying the patient with it.
The mattress works as both the patient support surface and the moving element of the transfer. Four layers make it work: memory e-fibre, an e-spring core, EVA foam, and a low-friction base.
A retractable rail that connects the bed to the stretcher. The snap-fit joint gives a physical lock and an audible click to confirm correct alignment before the transfer starts.
The lateral edges raise with a one-finger tap and release. In raised position, they create containment to stop the patient from rolling during transport.
A keyed lock at each rail joint. You have to physically verify these before the transfer begins. It's a deliberate mandatory step, not an optional one.
Transfer Protocol
Five steps. One caregiver.
For this to actually be used, one trained caregiver needs to complete it faster than two people doing the bedsheet method. That was the benchmark from day one.
Flatten the bed and lower the side railings. The swinging mechanism handles the mattress angle automatically, so there's no manual adjustment needed.
Line up the stretcher with the telescopic rail and extend it until the snap-fit joint locks into place. You'll hear it click.
Apply a steady lateral push. The low-friction base and the rail are designed to work together, so a single caregiver can manage this. The patient stays on the same surface throughout.
Use the one-finger tap-and-release to raise the side edges. This creates a lateral barrier to keep the patient from rolling during transport.
Physically verify all safety key locks. Detach the stretcher from the rail. The rail slides back to its stored position. Transfer done.
Reflections
What the project taught us.
The staff we spoke to weren't uninformed about the risks. Unsafe transfer has become the default simply because it's the fastest option available. A solution only holds up here if it makes the safe option easier than the current one.
Every existing transfer solution we found was built for a different context. The Indian public hospital has its own constraints: high patient volume, limited staff, tight budgets, and unpredictable infrastructure. It's not a lesser version of the Western hospital. It's a genuinely different operating environment, and the design needs to come from inside that context.
Getting to a five-step manual protocol honestly took more work than generating automated alternatives. A manual system that's reliably faster, needs no external power, and fails safely is harder to design than it sounds. Every decision had to account for the constraints.

Team
Group 4 · Design Thinking Studio · IIT Jodhpur · 2025